Essentials of Anatomy and Physiology for Nursing Practice
Student Resources
Answers to Revise Questions
What do the following terms mean?
Karyotype, Autosomes, Homologous chromosomes, Allele, Gene.
Ans: Karyotype: The display of chromosomes from a picture of a cell that have been cut out and arranged in pairs in order of size, with the two sex chromosomes at the end.
Autosomes: Those chromosomes in a cell which are not sex chromosomes.
Homologous chromosomes: The pair of chromosomes equivalent to each other.
Allele: An alternative form of the same gene at the corresponding position on the homologous chromosome.
Gene: A section of DNA which codes for a specific polypeptide chain.
Outline how the information carried on DNA is transcribed into RNA and translated into proteins.
Ans: The two strands of DNA separate to allow formation of the single-stranded messenger RNA (mRNA) molecule. The DNA which codes for a particular polypeptide molecule is transcribed into RNA, with each group of three bases in the DNA which code for an amino acid matched with the equivalent bases in RNA (with thymine in DNA replaced by uracil in RNA). The mRNA molecule moves out of the nucleus through the nuclear pores and links with a ribosome. The mRNA forms the template for translation into the polypeptide chain which becomes shaped into the protein. As the mRNA moves along the ribosome the amino acids coded for are attached to the growing polypeptide (protein) by transfer RNA (rRNA).
Describe the three Laws of Inheritance.
Ans: An organism with at least one dominant allele will display the effect of the dominant allele.
During gamete formation, the alleles for each gene segregate from each other, so that each gamete carries only one allele for each gene.
Genes for different traits can segregate independently during the formation of gametes.
Draw a Punnett Square to illustrate the genetic outcome from parents one of whom carries a dominant gene for a particular characteristic. What is the common pattern of descent through generations in such conditions?
Ans: One parent carries a dominant gene, for example, Huntingdon’s disease.
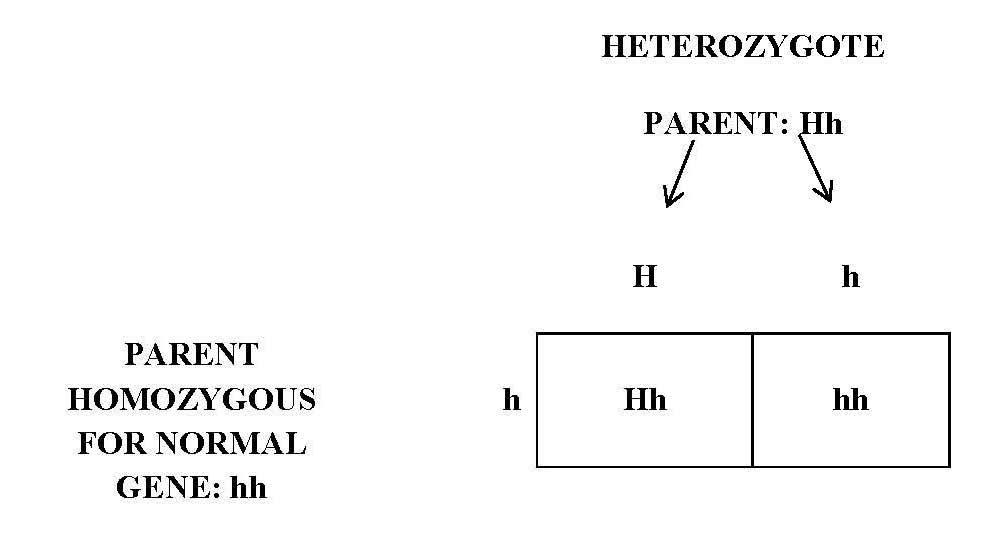
On average: 50% of offspring will carry one dominant gene.
50% will carry two normal genes.
Each baby has a 50% chance of carrying the dominant gene
The condition will normally appear in every generation.
Draw a Punnett Square to illustrate the genetic outcome from parents both of whom carry a recessive gene for a particular characteristic. What is the common pattern of descent through generations in such conditions?
Ans: Both parents are heterozygous for the abnormal gene, that is, each carries one copy of the gene (small c), for example, cystic fibrosis.
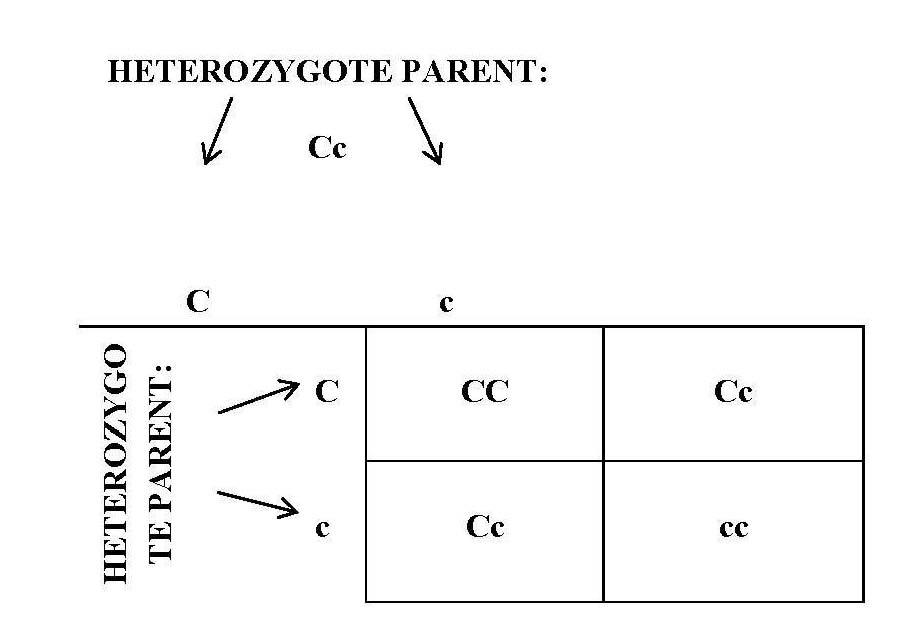
Possible offspring from two heterozygous parents:
- Homozygous for normal gene (CC): no disease occurs.
- Heterozygous (Cc): one normal and one abnormal gene, carriers of disease.
- Homozygous recessive (cc): two abnormal genes, have the disease.
The condition appears randomly in the family tree.
Case Study 1
What is the mode of inheritance of Duchenne muscular dystrophy?
Ans: X-linked recessive inheritance.
How likely is it that each further child by Jane and David will have the same condition?
Ans: Any girl baby is very unlikely to have the condition, but will have a 50% chance of being a carrier of the condition. Any boy baby will have a 50% chance of having the condition.
Briefly discuss the chances that Jane’s younger sister will have a boy or girl affected with this condition.
Ans: As their mother is almost certainly a carrier of cystic fibrosis (assuming that her brother had died of the disease), Jane’s younger sister will have a 50% chance of also being a carrier of the condition. If this is so, any girl baby she delivers will have a 50% chance of being a carrier, while a boy will have a 50% chance of having the condition. However, In-Vitro Fertilisation (IVF) with Preimplantation Genetic Diagnosis (PGD) can minimise this risk.
How does this condition affect the individual concerned?
Ans: Weakness of the legs and pelvis and loss of muscle mass are the first symptoms which usually occur between 2 and 3 years, but may start earlier. Muscle weakness spreads to arms, neck and other areas. Enlargement of certain muscles and difficulties in standing and climbing stairs occur and muscle tissue is later replaced by fibrous tissue. As the child gets older he will need braces to help in walking and will become wheelchair bound usually by about 12 years. Further loss of movement and other signs and symptoms develop. He is likely to die in his mid-twenties.
Case Study 2
How is Huntington’s disease inherited?
Ans: Autosomal dominant, with high penetrance (i.e., most people with the gene will show the condition).
If Dad has the gene for HD, what is the risk that I also carry it and the risk that I could pass it on to my daughter?
Ans: If her father has HD, this woman has a 50% chance that she carries the gene for Huntington’s disease. There is, thus, a 50% chance that she will pass it on to any child (son or daughter) that she has.
How can a family history be used with genetic testing to identify the risk of my brother’s children and extended family members developing HD? What are the potential difficulties involved for families?
Ans: A family history will provide information about the incidence of a condition which may be, or have been, HD. Genetic testing will enable living members of the family to have their status in relation to this gene to be identified. Those considering having children can now try out In-Vitro Fertilisation (IVF) with Preimplantation Genetic Diagnosis (PGD) to identify an embryo which does not carry the gene and thus they will be able to have a child without the risk of developing this condition in later life.
Older members of the family may not wish to know whether or not they carry this gene because nothing can be done anyway. All that testing will do is confirm that they will not develop the condition or that they are very likely to develop it. Some will feel that they would rather not know. The other issue that could arise is considering preparation for caring for those who are likely to develop HD.
Case Study 3
What is the mode of inheritance of cystic fibrosis and what proportion of the population carry the relevant gene?
Ans: Autosomal recessive. About one in 25 people of Northern European ancestry are carriers of this condition (with one gene) and about one in 2,500 to 3,000 babies are born with the condition (carrying two genes – one from each parent).
What is the risk that Jill carries the gene for cystic fibrosis?
Ans: As Jill’s mother has a brother with cystic fibrosis but she and her parents were healthy, her parents must both have been carriers of the condition. Thus Jill’s mother’s genetic makeup was:
1 in 4 of having the condition (she did not, thus risk eliminated);
2 in 4 of being a carrier;
1 in 4 of not having the gene for cystic fibrosis.
Thus she had a 2 in 3 chance of carrying this gene and because she passes one of her two genes at this site to her daughter, there is then a 1 in 2 chance that an abnormal gene is passed on.
Jill thus has a risk of ⅔ × ½ chance of carrying this gene = 1 in 3 risk.
How can Roger and Jill minimise the risk of having a child with cystic fibrosis?
Ans: Roger and Jill can both be tested for the abnormal gene. If only one of them carries it, any child they have may be a carrier but will not have the condition. It they both carry it, then any child has a 1 in 4 chance of having the condition. In this situation, they can have In-Vitro Fertilisation (IVF) with Preimplantation Genetic Diagnosis (PGD) to reduce the risk that the foetus will have the condition.